An article on an EMS blog caught my eye in the past week:
COPD was the third-leading cause of death in the U.S. in 2011 and is expected to become the third-leading cause of death worldwide by 2020.
Source:
Hoyert DL, Xu JQ. Deaths: preliminary data for 2011. Natl Vital Stat Rep, 2012; 61(6): 1–65.
Lopez AD, Shibuya K. Chronic obstructive pulmonary disease: current burden and future projections. Eur Respir J, 2006; 27(2): 397.
This caused me to dig up a presentation I did in 2006 at a Fitness Seminar, wherein I was discussing chronic medical conditions, which are caused by poor lifestyle choices and I noted then:
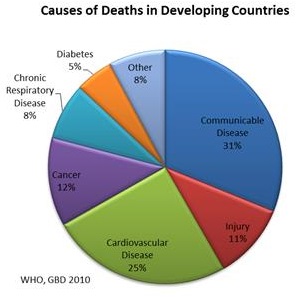
In 1999 CVD contributed to a third of global deaths. In 1999, low and middle income countries contributed to 78% of CVD deaths. By 2010 CVD is estimated to be the leading cause of death in developing countries. Heart disease has no geographic, gender or socio-economic boundaries.
I further stated:
Chronic illness have overtaken communicable disease as a major cause of death and disability worldwide. chronic diseases, including such noncommunicable conditions as cardiovascular disease, cancer, diabetes and respiratory disease, are now the major cause of death and disability, not only in developed countries, but also worldwide. The greatest total numbers of chronic disease deaths and illnesses now occur in developing countries.
I then dug deeper to see how this has changed since 2006, and the outlook has become even more bleak!
More than 75% of all deaths worldwide are due to noncommunicable diseases (NCDs). NCD deaths worldwide now exceed all communicable, maternal and perinatal nutrition-related deaths combined and represent an emerging global health threat. Every year, NCDs kill 9 million people under 60 years of age. The socio-economic impact is staggering. These NCD-related deaths are caused by chronic diseases, injuries, and environmental health factors. Important risk factors for chronic diseases include tobacco, excessive use of alcohol, an unhealthy diet, physical inactivity, and high blood pressure.
The world now suffers from a global epidemic of poor lifestyle choices! Medically we call them chronic illnesses or NCD’s, but the issue at hand is that they can be avoided, reversed and prevented; with smarter lifestyle choices. The why and the how of these lifestyle choices is a debate for another blog, but poor socioeconomic conditions, poverty, malnourishment and diets deficient in basic nutritional building blocks all form part of this dynamic.
These poor lifestyle choices and the death, illness, and disability they cause will soon dominate health care costs and should be causing public health officials, governments and multinational institutions to rethink how they approach this growing global challenge. To exacerbate the matter; the deaths, illnesses and disability are spiralling at even faster rates in the developing world, where the infrastructure is even weaker than in the developed world.
It is estimated that by 2020 the number of people who die from ischemic heart disease will increase by approximately 50% in countries with established market economies and formerly socialist economies, and by over 100% in low- and middle-income countries. Similar increases will also be found in cerebrovascular disease (Stroke) by 2020!
This is indeed a frightening prospect; NCDs are expected to account for 7 of every 10 deaths in the world! The overextended healthcare systems in Africa and Asia will battle to cope with these spiralling patient numbers.
A (positive) point to ponder as we consider this bleak outlook; the principal known causes of premature death from NCDs are tobacco use, poor diet, physical inactivity, and harmful alcohol consumption – all of these are preventable and manageable; as they relate to personal choices. Therefore we need to focus on creating a environment where these same individuals can make the correct choices which will have a positive impact on their lives. This is where governments, aid agencies and multi-nationals should focus their energies, and the approach should be more carrot than stick, which is not the case at present.
Reference’s:
http://apps.who.int/iris/bitstream/10665/128038/1/9789241507509_eng.pdf
